Family Medicine Associates 15 Walnut S Hamilton Ma
Abstract
Although myocarditis and pericarditis were not observed every bit adverse events in coronavirus affliction 2019 (COVID-nineteen) vaccine trials, there have been numerous reports of suspected cases following vaccination in the general population. We undertook a self-controlled case series study of people aged 16 or older vaccinated for COVID-xix in England between one December 2020 and 24 Baronial 2021 to investigate hospital admission or expiry from myocarditis, pericarditis and cardiac arrhythmias in the 1–28 days post-obit adenovirus (ChAdOx1, due north = 20,615,911) or messenger RNA-based (BNT162b2, north = 16,993,389; mRNA-1273, n = one,006,191) vaccines or a severe acute respiratory syndrome coronavirus ii (SARS-CoV-two) positive test (n = 3,028,867). Nosotros plant increased risks of myocarditis associated with the first dose of ChAdOx1 and BNT162b2 vaccines and the first and second doses of the mRNA-1273 vaccine over the i–28 days postvaccination period, and later a SARS-CoV-2 positive examination. Nosotros estimated an actress two (95% confidence interval (CI) 0, iii), one (95% CI 0, 2) and half-dozen (95% CI ii, 8) myocarditis events per one meg people vaccinated with ChAdOx1, BNT162b2 and mRNA-1273, respectively, in the 28 days following a starting time dose and an actress ten (95% CI 7, eleven) myocarditis events per one 1000000 vaccinated in the 28 days afterwards a 2nd dose of mRNA-1273. This compares with an extra 40 (95% CI 38, 41) myocarditis events per 1 meg patients in the 28 days following a SARS-CoV-2 positive test. We also observed increased risks of pericarditis and cardiac arrhythmias following a positive SARS-CoV-2 test. Like associations were not observed with whatsoever of the COVID-19 vaccines, apart from an increased adventure of arrhythmia following a 2d dose of mRNA-1273. Subgroup analyses by age showed the increased risk of myocarditis associated with the two mRNA vaccines was present but in those younger than 40.
Main
By the end of September 2021, more than than 6.3 billion doses of COVID-19 vaccination had been administered worldwide1. Clinical trials of COVID-19 vaccines were underpowered to detect the rare adverse events that are important for risk–benefit evaluations and to inform clinical practice postvaccination. Therefore, identifying such rare adverse events is now a global scientific priority.
As of four November 2021, there accept been i,783 reports to the United States Vaccine Adverse Result Reporting System (VAERS) of cases of heart inflammation, namely myocarditis or pericarditis, amidst people aged 12–29 years who received COVID-19 vaccines, in detail following mRNA vaccination, that is, BNT162b2 and mRNA-1273 vaccinestwo. Every bit of ix July 2021, the European Medicines Agency (EMA) has reported 145 cases of myocarditis and 138 cases of pericarditis out of 177 million doses of the BNT162b2 vaccine, and ix cases of myocarditis and xix cases of pericarditis out of twenty one thousand thousand doses of the mRNA-1273 vaccine3. In Israel, 275 cases of myocarditis were reported between Dec 2020 and May 2021 among more than v meg people vaccinated with the BNT162b2 vaccine4. No association betwixt ChAdOx1 vaccine and myocarditis or pericarditis has been reported. The same reports showed that these events are more probable to occur in adolescent and young adults, generally later on the second dose. Evaluation of the risks of adverse events following vaccination or SARS-CoV-2 infection in different age groups provides crucial information to determine whether the risks from the vaccine outweighs the risks following a positive SARS-CoV-ii test.
In England, the vaccination entrada began on 8 December 2020 with the BNT162b2 vaccine followed past the ChAdOx1 vaccine on 4 Jan 2021. In the get-go phase, priority was given to the most vulnerable, in a schedule based primarily on age. The mRNA-1273 vaccine became bachelor in England on 13 April 2021. Since vii April 2021, ChAdOx1 vaccine has non been recommended for individuals younger than 30 years of age, and since seven May 2021 for individuals younger than 40 years of age.
The English National Immunisation (NIMS) Database of COVID-nineteen vaccination includes information on vaccine type, date and doses for all people vaccinated in England. We linked NIMS, at individual patient level, to national data for mortality, hospital admissions and SARS-CoV-two infection data to examine the associations between the get-go and second dose of ChAdOx1, BNT162b2 or mRNA-1273 vaccines and cardiac agin events: myocarditis, pericarditis or cardiac arrhythmias. Nosotros used the same population to investigate the associations between a positive SARS-CoV-two test (before or after vaccination) as a secondary exposure and the aforementioned cardiac adverse events. We also assessed risks for the aforementioned outcomes post-obit vaccination or a SARS-CoV-2 positive test in younger persons (<40 years old). Incidence charge per unit ratios, the charge per unit of infirmary admission or death from each outcome in gamble periods subsequently vaccination or a positive test relative to baseline periods, were estimated using self-controlled example series (SCCS) methodology5,6.
Results
A total of 38,615,491 adults had been vaccinated with at least one dose of ChAdOx1 (n = 20,615,911), BNT162b2 (north = 16,993,389) or mRNA-1273 (north = ane,006,191) in England between 1 December 2020 and 24 August 2021 (Tabular array one). Of these, 32,095,748 had received two doses of either ChAdOx1 (n = 19,754,224, 95.8%), BNT162b2 (n = eleven,972,733, lxx.5%) or mRNA-1273 (north = 368,791, 36.7%). Individuals receiving the ChAdOx1 and BNT162b2 vaccine were older, on average, than those receiving the mRNA-1273 vaccine, as expected given that the mRNA-1273 vaccine roll-out began in Apr 2021 in the United Kingdom, when higher priority run a risk groups (including older people) had already received their vaccine.
Amongst those with at least one dose, there were three,028,867 (7.8%) individuals who had a SARS-CoV-two positive test. Of these, 2,315,669 (6.0%) individuals tested positive earlier vaccination; while 713,198 (1.eight%) and 298,315 (0.7%) tested positive after the first and second vaccine doses, respectively. Table 1 shows the characteristics of the study population, stratified by vaccine type and dose, and of those who tested positive for SARS-CoV-2.
During the written report menstruation there were one,615 and 1,574 admissions or deaths related to myocarditis and pericarditis, respectively (14 patients had both), and 385,508 related to cardiac arrhythmias. The characteristics of individuals with myocarditis, pericarditis and cardiac arrhythmias in the 1–28 days postvaccination differed by condition and according to the vaccine administered (Table 2). Supplementary Table 1 shows the characteristics of patients who died for the individual outcomes in the 1–28 days following a first or second dose of COVID-19 vaccine or SARS-CoV-2 infection. Table three and Fig. 1 testify the number of patients with upshot events in each exposure time flow and the incidence rate ratios (IRRs) and 95% CIs for outcomes in the exposure risk periods.

IRRs are presented for predefined risk periods (0, 1–7, 8–14, xv–21 and 22–28 days) after first or second dose of ChAdOx1, BNT162b2 and mRNA-1273 vaccines and a SARS-CoV-2 positive exam for the prerisk period (28 days earlier exposure). Horizontal bold line in each panel indicates 1.
Myocarditis
Of the 38,615,491 vaccinated individuals included in our report, 1,615 (0.004%) were admitted to hospital with, or died from, myocarditis at whatever time in the report period (either before or after vaccination); 397 (0.001%) of these occurred in the 1-28 days post whatsoever dose of vaccine. Of the 1,615 who were admitted or died, 359 (22.2%) had a SARS-CoV-ii positive exam, with 287 (17.8%) of these being earlier vaccination. At that place were 114 deaths with myocarditis recorded on the death certificate every bit a cause of expiry (23 had a SARS-CoV-2 positive test). Of those who have been admitted with, or died from, myocarditis in the one-28 days postvaccination, 12.7% (18) and 10.7% (nine) had a positive SARS-CoV-two test earlier the first and 2d dose ChAdOx1 vaccine, respectively, and seven.4% (7) before the beginning dose of BNT162b2 vaccine (Table two).
In that location was an increased risk of myocarditis at ane–7 days following the first dose of ChAdOx1 (IRR one.76; 95% CI 1.29, 2.42), BNT162b2 (IRR 1.45, 95% CI 0.97, two.12) and mRNA-1273 (IRR 8.38, 95% CI iii.53, 19.91), and the second dose of BNT162b2 (IRR 1.75, 95% CI 1.xiii, two.lxx) and mRNA-1273 (IRR 23.10, 95% CI half dozen.46, 82.56). There was an increased risk of myocarditis at i–7 days (IRR 21.08, 95% CI fifteen.34, 28.96), 8–14 days (IRR 11.29, 95% CI 7.70, sixteen.57), 15–21 days (IRR five.36, 95% CI 3.24, eight.89) and 21–28 days (IRR 3.08, 95%CI 1.65, 5.75) following a positive test.
Over the 1–28 days postvaccination, we observed an association with the first dose of ChAdOx1 (IRR 1.29, 95% CI 1.05, 1.58), BNT162b2 (IRR 1.31, 95% CI 1.03, 1.66) and mRNA-1273 (IRR two.97; 95% CI i.34, 6.58). Post-obit a 2d dose, the increased risk was much higher with mRNA-1273 (IRR ix.84, 95% CI two.69, 36.03) compared with BNT162b2 (IRR 1.thirty, 95% CI 0.98, 1.72). The risk of myocarditis was increased in the ane–28 days following a SARS-CoV-two positive exam (IRR 9.76, 95% CI 7.51, 12.69).
Pericarditis
Of the 38,615,491 vaccinated individuals included in our study, 1,574 (0.004%) were admitted to hospital with, or died from, pericarditis at any time in the study period (either earlier or afterward vaccination); 356 (0.001%) of these occurred in the 1-28 days after any dose of vaccine. Of the 1,574 who were admitted or died, 188 (11.9%) had a SARS-CoV-2 positive examination, with 154 (9.viii%) of these being before vaccination. There were 31 deaths with pericarditis recorded on the death document every bit crusade of death (half dozen had a SARS-CoV-ii positive test). Table 2 shows the percentages of patients with pericarditis events in the gamble catamenia who had a positive SARS-CoV-2 examination earlier vaccination by vaccine blazon and dose.
There were reduced risks of pericarditis subsequently a first dose of ChAdOx1 (IRR 0.59; 95% CI 0.37, 0.94 at 1–7 days, IRR 0.64; 95% CI 0.42, 0.99 at xv–21 days), of BNT162b2 (IRR 0.46; 95% CI 0.24, 0.ninety at eight–14 days) and post-obit a second dose of ChAdOx1 (IRR 0.49; 95% CI: 0.29, 0.82 at 22–28 days). In that location were insufficient numbers of events to evaluate associations with the mRNA-1273 vaccine by calendar week. There was an increased risk of hospital admission or death for pericarditis at 1–7 days (IRR 4.85, 95% CI 2.56, 9.eighteen) and 8–14 days (IRR 3.81, 95% CI one.90, 7.63) following a SARS-CoV-ii positive exam.
Over the one–28 days postvaccination, we observed a decreased risk of pericarditis post-obit the get-go dose of ChAdOx1 (IRR 0.74, 95%CI 0.59, 0.92), in contrast with an increased risk in the one–28 days post-obit a SARS-CoV-ii positive test (IRR ii.79, 95% CI 1.80, 4.32). No association was observed with the BNT162b2 or mRNA-1273 vaccine.
Cardiac arrhythmia
Of the 38,615,491 vaccinated individuals included in our study, 385,508 (ane.0%) were admitted to hospital with or died from cardiac arrhythmia at whatsoever time in the written report period (either before or afterwards vaccination); 86,754 (0.2%) of these occurred in the 1-28 days subsequently any dose of vaccine. Of those who were admitted or died 39,897 (10.3%) had a SARS-CoV-2 positive exam, with 29,694 (7.7%) having a positive examination before vaccination. There were 7,795 deaths with cardiac arrhythmia recorded equally the cause of decease (1,108 had a SARS-CoV-two positive test). Table 2 shows the percentages of patients with cardiac arrhythmia events in the risk period who had a positive SARS-CoV-2 test earlier vaccination by vaccine type and dose.
In that location were decreased risks of cardiac arrhythmia after the commencement dose of ChAdOx1 (IRR 0.95, 95% CI 0.92, 0.97 at 1–7 days and over subsequent periods) and BNT162b2 (IRR 0.79, 95% CI 0.76, 0.81 at 1–vii days and over subsequent periods) and following a second dose of ChAdOx1 (IRR 0.84, 95% CI 0.82, 0.87 at 1–7 days; IRR 0.97, 95% CI 0.94, 0.99 at eight–14 days) and of BNT162b2 (IRR 0.85, 95% CI 0.83, 0.88 at 1–vii days; IRR 0.95, 95% CI 0.92, 0.98 at 8–15 days). There was an increased take chances of cardiac arrhythmia following a second dose of mRNA-1273 (IRR ane.93, 95% CI 1.25, ii.96 at 1–7 days) and at 1–7 days (IRR 11.73, 95% CI 11.33, 12.14), 8–xiv days (IRR half-dozen.57, 95%CI 6.30, half-dozen.85), 15–21 days (IRR 2.30, 95% CI 2.15, 2.45) and 21–28 days (IRR 1.67, 95% CI 1.55, 1.80) post-obit a SARS-CoV-ii positive exam.
Over the ane–28 days post vaccination, nosotros found a decreased adventure of cardiac arrhythmia associated with a first dose of ChAdOx1 (IRR 0.94, 95% CI 0.93, 0.96) and BNT162b2 (IRR 0.89, 95% CI 0.87, 0.xc) and following a 2nd dose of ChAdOx1 (IRR 0.95, 95% CI 0.94, 0.96) and BNT162b2 (IRR 0.95, 95% CI 0.93, 0.96). At that place was an increased gamble of cardiac arrhythmia following a 2d dose of mRNA-1273 (IRR i.46, 95% CI, 1.08, i.98) and a SARS-CoV-2 positive test (IRR 5.35, 95% CI 5.21, 5.50).
Subgroup analyses by age group and sex
Table 4 shows the IRRs for the outcomes in the overall one–28 day risk periods before and later on each exposure past sex and in those aged under xl years or 40 years and older. Supplementary Tables two and 3a show the IRRs estimated for each week in the 1–28 days following exposure in these subgroups. Whilst the findings more often than not mirrored those reported in the overall one–28 day menstruum in each subgroup, given the small numbers of events in some weeks, care is needed in the interpretation. Here, we written report the results of the subgroup analyses only for myocarditis.
In those aged under xl years, we observed increased risks of myocarditis in the 1–28 days post-obit a first dose of BNT162b2 (IRR 1.83, 95% CI i.20, 2.79) and of mRNA-1273 (IRR 3.89, 95% CI 1.60, nine.44), after a second dose of BNT162b2 (IRR three.40, 95% CI 1.91, 6.04) and of mRNA-1273 (IRR 20.71, 95% CI four.02, 106.68) and following a SARS-CoV-two positive test (IRR 4.06, 95%CI 2.21, seven.45). No association was found with the ChAdOx1 vaccine. In those anile xl years or older, the take a chance of myocarditis was increased in the 1–28 days following a first dose of ChAdOx1 (IRR 1.33, 95% CI 1.06, 1.67) and a SARS-CoV-2 positive test (IRR 12.18, 95% CI 9.01, sixteen.46). No clan was found with the BNT162b2 vaccine and numbers of events were insufficient to evaluate associations with the mRNA-1273 vaccine.
In women, we found an increased risk of myocarditis 1–28 days following a commencement dose of ChAdOx1 (IRR one.forty, 95% CI ane.01, 1.93) and BNT162b2 (IRR 1.54, 95% CI 1.08, ii.20), and following a SARS-CoV-2 positive test (IRR 11.00, 95% CI 7.12, xvi.99). There were bereft numbers of events to evaluate associations with the mRNA-1273 vaccine for women. In men, we found an increased risk of myocarditis at 1–28 days post-obit a first and 2nd dose of mRNA-1273 (IRR 3.79, 95% CI 1.59, ix.04 and IRR 12.27, 95%CI two.77, 54.37, respectively) and following a SARS-CoV-2 positive test (IRR 9.06, 95% CI half-dozen.51, 12.62). No clan was found with the ChAdOx1 or BNT162b2 vaccines.
Supplementary Tabular array 3b shows the IRRs of these outcomes estimated in the 1–28 days following exposure when restricting to unlike age groups (16–29, 29–39 and 40 plus years). The increased take a chance of myocarditis associated with either messenger RNA-based vaccine consistently occurs in the younger population (<40 years).
Subgroup analyses past previous SARS-CoV-2 infection
Supplementary Table iv shows the estimated IRRs for myocarditis, pericarditis or cardiac arrhythmias in the 1–28 24-hour interval adventure period later each vaccination in those who did not have a SARS-CoV-two positive test before vaccination. These results generally agreed with the main analyses. We did not observe any increased risk of myocarditis, pericarditis or arrhythmia following a first or second dose of ChAdOx1 or BNT162b2 vaccine in those who tested positive before vaccination, only in that location was a decreased risk of cardiac arrythmias following a first dose of either vaccine (Supplementary Table 5). There were insufficient numbers of events to evaluate associations with the mRNA-1273 vaccine in this subgroup.
Subgroup analyses past categories of cardiac arrhythmia
Cardiac arrhythmias (n = 385,508) were categorized every bit atrial fibrillation or palpitate (n = 229,248, 59.four%), atrio-ventricular (AV) block and related conduction disorders (n = 114,701, 29.vii%), ventricular tachycardia (due north = 8,211, 2.i%), ventricular fibrillation (n = 2,910, 0.vii%) and other, including supraventricular tachycardia (n = 130,485, 33.viii%).
Over the ane–28 days postexposure, we observed an increased risk of atrial fibrillation or flutter arrhythmia at xv–21 days following a first dose of mRNA-1273 vaccine (IRR ii.06, 95% CI 1.eleven, 3.82); of ventricular fibrillation at 22–28 days following a second dose of ChAdOx1 vaccine (IRR 1.35, 95% CI i.05, one.74) and of other cardiac arrhythmia at 1–7 days following a second dose of mRNA-1273 vaccine (IRR ii.32, 95% CI 1.49, 3.62). There was an increased risk of all cardiac arrhythmia subgroups in the one–28 days following a SARS-CoV-two positive examination (Supplementary Table 6).
Robustness of results
We constitute no increased risk of celiac disease (negative control) across the prespecified time periods for the vaccine exposures, with the exception of the 15–21 days after the second dose of ChAdOx1 (IRR one.20; 95% CI: ane.05, 1.36). We besides establish a decreased take chances on the day of vaccination, as expected given the healthy vaccinee issue. Anaphylaxis (positive control) showed the expected increased hazard on the twenty-four hour period of vaccination (both beginning and 2nd dose), but non at afterward periods following the ChAdOx1 and BNT162b2 vaccinations (Supplementary Table seven). There were insufficient numbers of events to evaluate associations between anaphylaxis and the mRNA-1273 vaccine. Run across Methods for description of the selection of controls outcomes.
Supplementary Table 8a and Extended Data Figs. ane–three show the results for several sensitivity analyses. Overall, our chief findings were non sensitive to censoring due to expiry, and IRRs for the second dose of vaccination agree with main results when we removed those who had the outcome later on the offset dose of any vaccine, only earlier the second.
As expected, sensitivity analyses 6–8 testify that, by reducing the length of the prerisk flow, we could exaggerate the relative incidence associated with vaccine exposure and understate the relative incidence associated with infection exposure, whereas increasing the length of the prerisk catamenia has the contrary effect (Supplementary Table 8b).
A sensitivity analysis restricting the report catamenia up to 17 May 2021, when the Centres for Disease Control and Prevention (CDC) announced cases of myocarditis later the BNT162b2 vaccine, showed no increased incidence of myocarditis in the 1–7 days following a second dose of BNT162b2 (IRR 1.07, 95% CI 0.59, 1.97). The historic period distribution of those vaccinated with ChAdOx1 in these two time periods was similar, simply those vaccinated with BNT162b2 were older in the restricted study menstruation (13.8% versus 29.7% were younger than 40 years; Supplementary Tabular array 9).
Hospital duration of stay for myocarditis
The median hospital elapsing of stay for those with myocarditis in the 28 days postvaccination was 3 days (interquartile range (IQR): 1, 9) for ChAdOx1, iii days (IQR: 1, 7) for BNT162b2 and 4 days (IQR: iii, 6) for mRNA-1273, with means of eight.iii, v.vii and 4.v days, respectively. This compares with a median of 4 days (IQR: 1, nine) and mean of seven.6 days for those whose admissions had not occurred in the 28 days postal service vaccination.
Accented measures of issue of vaccination and SARS-CoV-two infection
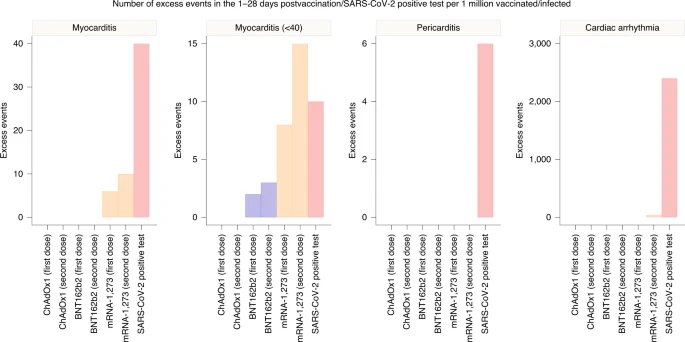
We estimated the number of exposures needed for ane excess event and the excess number of events per i million exposed for each outcome (Fig. 2 and Supplementary Table 10). In the 1–28 days following the first dose of the ChAdOx1, BNT162b2 and mRNA-1273 vaccine, an actress two (95% CI 0, 3), one (95%CI 0, 2) and six (95% CI two, viii) myocarditis events per one million exposed would be predictable, respectively. In the one–28 days post-obit the second dose of mRNA-1273, an extra x (95% CI 7, eleven) myocarditis events per 1 meg persons would exist anticipated. This compares with an extra 40 (95% CI 38, 41) myocarditis events per i million in the 1–28 days following a SARS-CoV-2 positive examination.
When IRR did not show a significant increment of incidence over the 1–28 days postvaccination or a SARS-CoV-2 positive test, absolute measures are not given.
Subgroup analyses by age showed that the increased take chances of events associated with the ii mRNA vaccines was present only in those aged under forty years. For this age group, we estimated two (95% CI 1, 3) and 8 (95%CI 4, ix) excess cases of myocarditis per ane meg people receiving a first dose of BNT162b2 and mRNA-1273, respectively, and 3 (95% CI 2, four) and 15 (95%CI 12, xvi) backlog cases of myocarditis per 1 million people receiving a second dose of BNT162b2 and mRNA-1273, respectively. This compares with ten (95% CI 7, 11) actress cases of myocarditis following a SARS-CoV-ii positive exam in those aged under twoscore years.
Discussion
This is the largest study to appointment of astute cardiac outcomes after SARS-CoV-two vaccination or infection, the first to compare the adventure of cardiac events between different vaccine products and SARS-CoV2 infection and the outset to investigate the association between cardiac events and the ChAdOx1 vaccine.
Our findings are relevant to the public, clinicians and policy makers. First, at that place was an increase in the hazard of myocarditis within a week of receiving the first dose of both adenovirus and mRNA vaccines, and a higher increased chance subsequently the second dose of both mRNA vaccines. In dissimilarity, we found no show of an increase in the risk of pericarditis or cardiac arrhythmias following vaccination, except in the one–28 days following a second dose of the mRNA-1273 vaccine. Second, in the same population, at that place was a greater risk of myocarditis, pericarditis and cardiac arrhythmia following SARS-CoV-two infection. Third, the increased risk of myocarditis afterwards vaccination was higher in persons aged under 40 years. We estimated extra myocarditis events to exist between ane and ten per 1000000 persons in the month following vaccination, which was substantially lower than the xl extra events per 1000000 persons observed following SARS-CoV-ii infection.
We assessed the temporal clan between COVID-19 vaccination and cardiac adverse events using hospital admissions with diagnoses of myocarditis or pericarditis, and cardiac arrhythmias. Myocarditis is an inflammatory disorder of the myocardium that commonly results from viral infection, systemic immune-mediated diseases or immunomodulatory treatmentsseven. It occurs more normally in men, which may be a issue of dissimilar furnishings of sexual practice hormones on the immune systemviii. Several cases take been reported in patients hospitalized with SARS-CoV-2 infection, and screening for cardiac involvement using cardiac troponin testing has demonstrated that myocardial injury is mutual and associated with poor outcomes9. Irrespective of the underlying etiology of myocarditis, those who develop important ventricular harm are at increased take chances of cardiogenic shock and mortality10, highlighting the importance of ascertaining whether myocarditis may exist temporally associated with vaccination for SARS-CoV-two.
Whereas myocarditis is a specific form of cardiac inflammation, pericarditis reflects inflammation localized to the pericardium, and the occurrence of cardiac arrhythmias, although associated with both, is not a specific indictor of cardiac inflammation. Thus, neither pericarditis nor any category of cardiac arrhythmia were associated specifically with COVID-19 vaccination10,11,12. Myocarditis is underdiagnosed in practise13, with clinical bias being directed towards myocardial ischemia or infarction. Thus, our use of diagnostic codes for myocarditis from routine data suggest that the ascertainment of cardiac inflammation later on COVID-19 vaccination is likely to be under- rather than over-represented14,15.
Although no cases of myocarditis were observed in the randomized trials of vaccine, this status is uncommon, and postmarket authorization surveillance may be required. Our observation of an increased hazard within 7 days of receiving the vaccine is consistent with the presentation of viral myocarditis, where viral symptoms are often reported in the calendar week leading up to presentation. Furthermore, myocarditis following vaccination has been reported with other vaccines, for case, in healthy adults after receipt of alive vaccinia virus vaccinessixteen,17 Whilst the mechanisms of myocarditis following exposure to SARS-CoV2 infection and vaccination are not known, information technology seems likely that systemic complications of infection are a consequence of an immune-mediated, virus-independent immunopathologic processeighteen. Nevertheless, vaccine mediated expression of SARS-CoV-2 surface spike protein on the surface of cardiomyocytes could potentially trigger an immunologic response resulting in organ-specific cell death19,20
Our findings are consistent with those from a instance-control study of 884,828 persons receiving the BNT162b2 vaccine in Israel21. That written report observed an association with myocarditis in the 42 days post-obit vaccination (risk ratio of iii.24), but no association with pericarditis or cardiac arrhythmia. Two further studies from Israel add to our observations by providing clinical review to ensure robust case ascertainment22 and reporting investigations and outcomes in individual patients with myocarditis following the BNT162b2 vaccine23. Witberg et al.21,22 observed a small excess in events 3–5 days following the 2d dose of BNT162b2 vaccine, but nearly were mild presentations and simply one classified equally fulminant22. Mevorach et al. observed an incidence ratio of 5.34 for myocarditis in five,442,696 persons following BNT162b2, although this was attenuated when restricted to the 136 definite and probable cases of myocarditis23. Hazard of myocarditis was restricted to males under the historic period of forty years and merely observed following the second dose. Similarly, ii studies from the United States take reported an incident rate ratio of 2.7 for myocarditis in the 10 days post-obit the second dose of both mRNA vaccines24 and an estimated 6.three and ten.1 extra cases per meg doses in the 1- to 21-solar day period following the showtime and 2nd dose of both mRNA vaccines, respectively, in those younger than 40 years25.
Our findings extend these observations by including 38 million adults in England receiving both mRNA and adenovirus-mediated vaccine. At that place were i,615 myocarditis events in our written report population, enabling a granular evaluation of subgroups and the temporal association in the weeks post-obit vaccination. We observed a small backlog in myocarditis events later on both the outset and second dose of vaccine, but this risk was restricted to a 7-mean solar day flow following vaccination. This observation was not limited to the mRNA vaccines equally we also found an excess in myocarditis events following the outset dose of ChAdOx1 vaccine. The backlog risk was observed in men and women but was only consistently observed following both mRNA vaccines in those younger than 40 years, although this may, in part, reverberate the small number of individuals over the age of 40 years receiving the mRNA-1273 vaccine in England.
Whilst myocarditis can be life-threatening, most vaccine-associated myocarditis events have been mild and self-limiting22. The gamble observed here is small and confined to the 7-day period following vaccination, whereas the lifetime adventure of morbidity and mortality following SARS-CoV-2 infection is substantial. Indeed, myocardial injury is very common in persons admitted to hospital with SARS-CoV-2 infection26, when evaluated systematically using high-sensitivity cardiac troponin tests27. Moreover, evidence of myocardial injury, irrespective of whether due to myocarditis or myocardial ischemia, is associated with a college risk of in-hospital death28. We judge that the absolute number of backlog myocarditis events in the 28 days following a first dose of adenovirus or mRNA vaccine is between one and six per million persons vaccinated, and the excess risk following the second dose of the mRNA-1283 vaccine is ten per million. By contrast, nosotros guess 40 excess myocarditis events per million in the 28 days following SARS-CoV-2 infection. The risks are more evenly counterbalanced in younger persons aged up to 40 years, where we estimated the excess in myocarditis events following SARS-CoV-2 infection to be 10 per million with the excess following a second dose of mRNA-1273 vaccine beingness 15 per one thousand thousand. Further research is required to understand why the risk of myocarditis seems to be higher post-obit mRNA-1273 vaccine. Although the wider societal benefits of controlling the spread of virus to those who are more vulnerable are substantial, these data may help inform public wellness policy and the choice of vaccine offered to younger adults.
This study has several strengths. First, the United Kingdom offered an ideal place to carry out this study given that iii vaccinations have been rolled out at speed and calibration. 2d, this was a population-based study of data recorded prospectively and avoided remember and choice biases linked to case reports. Third, the big sample size provided sufficient power to investigate these rare outcomes, which could not be assessed through clinical trials. Fourth, the SCCS written report design removes potential confounding from stock-still characteristics, and the breakdown of our report catamenia into weekly blocks deemed for temporal misreckoning. Of note, the estimated IRRs are consistently less than 1 in the pre-exposure period before vaccination and greater than 1 in the prerisk period before a SARS-CoV-ii positive test. This was expected since events are unlikely to happen shortly before vaccination (relatively healthy people are receiving the vaccine) and more likely to happen earlier a SARS-CoV-2 positive test (as a standard procedure, patients admitted to hospital are tested for SARS-CoV-2). We too assessed the robustness of our results through analyses of command outcomes and several sensitivity analyses.
There are some limitations that we should acknowledge. Offset, although we used an established methodology for evaluating vaccine safety, nosotros cannot determine whether our findings are causal. Second, we relied on hospital admission codes and death certification to define our outcome measures. As such, we are non able to decide what proportion of patients underwent cardiac imaging or biopsy to confirm the diagnosis of myocarditis. It remains possible that our findings have been influenced by referral bias, with troponin testing performed more than widely following vaccination due to media reports of vaccine-associated myocarditis. Our sensitivity analysis restricted to those persons vaccinated earlier the CDC announcement does not disbelieve this possibility, although the different results could too be explained by the fact that the population who received the BNT162b2 vaccine were older in the restricted study period. Third, the mRNA-1273 vaccine roll-out began in April 2021 in the United Kingdom; as a consequence, the number of events in patients who received this vaccine was low. Although the signal associated with myocarditis is stiff for this vaccine, intendance is needed in the interpretation, and it would be useful to replicate our results in similarly large datasets internationally. Fourth, we are unclear near the biological plausibility of the observed reduced risks of pericarditis and arrhythmia linked to vaccination and, although these findings are consequent of those of Barda et al.21, they should be interpreted with circumspection. 5th, in this study, nosotros performed several comparisons, which may atomic number 82 to some erroneous inferences. Every bit a result, careful interpretation is needed, especially for the borderline associations establish. Finally, information technology is as well of import to note that command outcomes were chosen to appraise the validity of the association between cardiac adverse events and vaccination. Control outcomes for a SARS-CoV-ii positive test are more challenging to find, as the unabridged health system is affected by the pandemic. Caution is needed in interpretation of the findings for a SARS-CoV-2 positive test in light of this.
In summary, this population-based study quantifies for the first time the risk of several rare cardiac agin events associated with 3 COVID-19 vaccines too as SARS-CoV-ii infection. Vaccination for SARS-CoV-two in adults was associated with a pocket-size increase in the risk of myocarditis within a calendar week of receiving the first dose of both adenovirus and mRNA vaccines, and subsequently the second dose of both mRNA vaccines. By contrast, SARS-CoV-2 infection was associated with a substantial increment in the take a chance of hospitalization or death from myocarditis, pericarditis and cardiac arrhythmia.
Methods
Ethical blessing
National Health Service Research Ethics Committee approval was obtained from East Midlands-Derby Inquiry Ethics Committee [reference 04/03/2021].
Data
We used the National Immunisation Database (NIMS) database of COVID-19 vaccination to identify vaccine exposure. This includes vaccine blazon, appointment and doses for all people vaccinated in England. Nosotros linked NIMS vaccination data, at individual level, to national data for mortality (Office for National Statistics), hospital admissions (Infirmary Episode Statistics) and SARS-CoV-2 infection data (Second Generation Surveillance System).
Written report design
The SCCS design was used; this pattern was developed originally to examine vaccine safetyfive,6. The analyses are provisional on each case, and so whatsoever fixed characteristics during the study period, such as sexual activity, ethnicity or chronic weather, are inherently controlled for. Any time-varying factors, like seasonal variation, need to exist adapted for in the analyses.
Report period and population
Nosotros examined the associations between ChAdOx1, BNT162b2 or mRNA-1273 vaccines and selected cardiac conditions during the ongoing COVID-xix vaccination programme in England, which commenced on 8 December 2020. Divide analyses were carried out in cases with each cardiac issue of interest. People were considered eligible for inclusion in each study accomplice if they had received at least ane vaccine dose, were at to the lowest degree 16 years old and were admitted to hospital with, or died from, the result of interest between i Dec 2020 and 24 August 2021 (concluding data update). Patients were followed up from the written report start (one Dec 2020) to the earliest of the stop of the report menses or when they died. Patients with a hospital admission for the aforementioned outcome in the two years before the start of the study period were excluded.
Outcomes
The outcomes in this report are selected cardiac conditions with previous indications of clan with SARS-CoV-2 infection or COVID-19 vaccination. These included myocarditis, pericarditis and arrythmia. We used the International Classification of Diseases-10 codes to ascertain each outcome, as listed in Supplementary Table xi. The outcomes were identified as the first infirmary admission due to the event of involvement, or death recorded on the expiry certificate with the International Classification of Diseases-10 lawmaking related to the outcome of interest within the study period. A histogram showing the number of admissions in England from 1 April 2019 to 24 August 2021 is presented in Extended Data Fig. 4.
Exposures
The exposure variables were a first or 2nd dose of the ChAdOx1, BNT162b2 or mRNA-1273 vaccines, or SARS-CoV-two infection, defined as the kickoff SARS-CoV-2 positive examination in the written report period. All exposures were included in the same model. We divers the exposure risk intervals equally the following prespecified time periods: 0, 1–7, 8–xiv, 15–21 and 22–28 days subsequently each exposure date, under the assumption that the adverse events nether consideration are unlikely to exist related to exposure later than 28 days postexposure. We assumed that the risks may exist different after each vaccine dose (first and 2nd), and hence we allowed for a dose consequence, by defining a carve up risk interval after each dose: 0, 1–7, 8–14, 15–21 or 22–28 days later the start dose and 0, 1–7, 8–14, xv–21 or 22–28 days later the second dose. To avert overlapping chance periods, we assumed that later on exposures (2d dose) have precedence over before ones (start dose), except for the 28-day prerisk period for the second dose, as shown in Extended Information Fig. 5. A prerisk interval of 1–28 days earlier each exposure date was included to account for potential bias that might arise if the occurrence of the outcome temporarily influenced the likelihood of exposure. The baseline period for the vaccination exposures comprised the remaining time from 1 December 2020 until 29 days before the showtime dose date and from 29 days after the offset dose until 29 days before the second dose (if applicable), and from 29 days later on the second dose until 24 Baronial 2021 or the censored appointment if earlier. A SARS-CoV-2 positive test was considered every bit a split up exposure in the models, which allowed overlapping risk windows with vaccination exposure.
Seasonality and COVID-xix pandemic menstruation
Hospital admissions were likely influenced by the pressure on the health systems due to COVID-19, which was not compatible during the pandemic catamenia. To allow for these underlying seasonal effects, we divide the study observation flow into weeks and adjusted for week every bit a cistron variable in the statistical models.
Statistical assay
We described characteristics of each accomplice (vaccinated patients with the outcomes of interest) in terms of age, sex and ethnic group. The SCCS models were fitted using a provisional Poisson regression model with an offset for the length of the exposure adventure period. Divide analyses were carried out for each cardiac outcome of interest. IRR, the relative charge per unit of hospital admissions or deaths due to each outcome of interest in exposure risk periods relative to baseline periods, and their 95% CI were estimated by the SCCS model adjusted for calendar week equally a time-varying covariate. Exposure terms for vaccines and for a SARS-CoV-2 positive exam were included in the same model.
We investigated if the associations betwixt vaccine exposures and outcomes are sex- or historic period-dependent by running subgroups analyses amongst those aged nether 40 years and those aged 40 years and older and by gender. We also conducted analyses restricted to those with a SARS-CoV-2 infection before vaccination and those without SARS-CoV-2 infection. Finally, we performed subgroup analyses by prespecified categories of cardiac arrythmia every bit reported in Supplementary Table 11.
We conducted sensitivity analyses to appraise the robustness of results to assumptions, such as that the occurrence of an consequence event did non influence the probability of subsequent exposures by (1) excluding those who died from the outcome and (two) restricting analysis to the period postvaccination, without censoring at death. To assess potential reporting delays in the data by (iii) restricting the report to the period upwardly to 1 August 2021. To include only fourth dimension unaffected by any notoriety bias by (4) restricting the written report to the period up to 17 May 2021, when CDC announced cases of myocarditis later on BNT162b2 vaccine and (five) removing patients who had outcomes in the 28 days afterwards a starting time dose, but before a 2nd dose, since they are less likely to have a 2nd dose if they experienced an agin event subsequently the beginning.
To compare the choice of different pre-exposure risk periods, we as well included three extra sensitivity analyses using unlike lengths for the prerisk period: (6) including the prerisk menstruation in the baseline, (7) including only the 1–14 days earlier exposure in the prerisk flow and (8) including a longer prerisk period of 59 days.
Stata five.17 was used for these analyses.
Absolute risk
Absolute run a risk differences cannot be obtained using SCCS. We supplemented our estimates of IRRs with measures of event using a method29 adult to estimate the number of exposures needed to produce one backlog adverse outcome and the excess number of events per 1 million exposed for each outcome.
SCCS assumptions
Independence between outcome and exposure
We causeless that patients who experienced an outcome earlier vaccination were likely to delay vaccination until symptoms had improved. Therefore, we included a prerisk period in the analyses, lasting from ane to 28 days before vaccination, which removes this menstruation from the baseline period (Extended Information Fig. 6). Infirmary admissions for the events of involvement tin trigger COVID-nineteen testing. Such events may well be caused past SARS-CoV-2 infection, but the reverse causality involved in their detection induces bias. To reduce the bias, which could over or underestimate the effect of infection, we decided to allocate day 0 to a risk period on its own30.
Result-dependent observation periods
We tested this assumption with sensitivity analyses 1 and 2. These further analyses agreed with the main analysis, suggesting that there should be little concern for these outcomes.
Negative and positive control outcomes
We examined the association of exposures with celiac disease as a negative control outcome31, which is assumed not to be associated with exposure to vaccination or SARS-CoV-two infection; and with anaphylaxis as a positive control outcome given that information technology could occur shortly subsequently vaccination with either vaccine32.
Reporting Summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Information availability
The data that support the findings of this study—NIMS Database of COVID-19, mortality (Role of National Statistics), hospital admissions (Infirmary Episode Statistics) and SARS-CoV-2 infection data (PHE)—are not publicly available because they are based on deidentified national clinical records. Due to national and organizational data privacy regulations, private-level information such as those used for this study cannot be shared openly.
Lawmaking availability
The code used for this written report has been deposited in the git repository of the research group, which is protected past privacy. Admission to the code is available from the authors on request for noncommercial, academic and inquiry use only.
References
-
Number of people vaccinated confronting COVID-19. Our World in Data; https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2021-09-30&facet=none&pickerSort=asc&pickerMetric=location&Metric=People+vaccinated+%28by+dose%29&Interval=7-solar day+rolling+average&Relative+to+Population=false&Align+outbreaks=false&country=~ITA (2021).
-
Selected adverse events reported after COVID-nineteen vaccination. Centers for Disease Control and Prevention; https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html (2021).
-
Comirnaty and Spikevax: possible link to very rare cases of myocarditis and pericarditis. European Medicines Agency; https://world wide web.ema.europa.eu/en/news/comirnaty-spikevax-possible-link-very-rare-cases-myocarditis-pericarditis (2021).
-
Surveillance of myocarditis (inflammation of the heart musculus) cases betwixt December 2020 and May 2021 (including). Ministry building of Health of the Israeli Regime; https://www.gov.il/en/departments/news/01062021-03 (2021).
-
Petersen, I., Douglas, I. & Whitaker, H. Cocky controlled case series methods: an alternative to standard epidemiological report designs. Brit. Med. J. 354, i4515 (2016).
-
Farrington, C. P., Nash, J. & Miller, Eastward. Example series assay of adverse reactions to vaccines: a comparative evaluation. Am. J. Epidemiol. 143, 1165–1173 (1996).
-
Pollack, A. et al. Viral myocarditis–diagnosis, treatment options, and current controversies. Nat. Rev. Cardiol. 12, 670–680 (2015).
-
Fairweather, D., Cooper, L. T. & Blauwet, L. A. Sex and gender differences in myocarditis and dilated cardiomyopathy. Curr. Probl. Cardiol. 38, 7–46 (2013).
-
Chapman, A. R., Bularga, A. & Mills, Northward. L. High-sensitivity cardiac troponin tin be an ally in the fight confronting COVID-19. Circulation 141, 1733–1735 (2020).
-
Kociol, R. D. et al. Recognition and initial direction of fulminant myocarditis: a scientific statement from the American Heart Association. Apportionment 141, e69–e92 (2020).
-
Friedrich, M. G. et al. Cardiovascular magnetic resonance in myocarditis: a JACC white paper. J. Am. Coll. Cardiol. 53, 1475–1487 (2009).
-
Ferreira, V. G. et al. Cardiovascular magnetic resonance in nonischemic myocardial inflammation: expert recommendations. J. Am. Coll. Cardiol. 72, 3158–3176 (2018).
-
Pasupathy, S. et al. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation 131, 861–870 (2015).
-
Dastidar, A. G. et al. Prognostic role of CMR and conventional risk factors in myocardial infarction with nonobstructed coronary arteries. JACC Cardiovasc. Imaging 12, 1973–1982 (2019).
-
Kim, J. Y., Han, Grand. & Suh, Y. J. Prevalence of aberrant cardiovascular magnetic resonance findings in recovered patients from COVID-19: a systematic review and meta-analysis. J. Cardiovasc. Magn. Reson. 23, 100 (2021).
-
Mei, R. et al. Myocarditis and pericarditis after immunization: gaining insights through the Vaccine Agin Event Reporting System. Int. J. Cardiol. 273, 183–186 (2018).
-
Engler, R. J. et al. A prospective study of the incidence of myocarditis/pericarditis and new onset cardiac symptoms following smallpox and influenza vaccination. PLoS ONE 10, e0118283 (2015).
-
Dorward, D. A. et al. Tissue-specific immunopathology in fatal COVID-nineteen. Am. J. Respir. Crit. Care Med. 203, 192–201 (2021).
-
Bozkurt, B., Kamat, I. & Hotez, P. J. Myocarditis with COVID-19 mRNA vaccines. Circulation 144, 471–484 (2021).
-
Makunts, T. et al. Myocarditis occurrence with cancer immunotherapy beyond indications in clinical trial and post-marketing data. Sci. Rep. 11, 17324 (2021).
-
Barda, North. et al. Condom of the BNT162b2 mRNA Covid-19 vaccine in a nationwide setting. North. Engl. J. Med. 385, 1078–1090 (2021).
-
Witberg, Chiliad. et al. Myocarditis afterward Covid-19 vaccination in a big health care system. N. Engl. J. Med. https://doi.org/ten.1056/NEJMoa2110737 (2021).
-
Mevorach, D. et al. Myocarditis subsequently BNT162b2 mRNA vaccine against Covid-19 in Israel. Northward. Engl. J. Med. https://doi.org/10.1056/NEJMoa2109730 (2021).
-
Simone, A. et al. Acute myocarditis following COVID-19 mRNA vaccination in adults aged 18 years or older. JAMA Intern. Med. https://doi.org/10.1001/jamainternmed.2021.5511 (2021).
-
Klein, N. P. et al. Surveillance for adverse events subsequently COVID-19 mRNA vaccination. JAMA 326, 1390–1399 (2021).
-
Sandoval, Y., Januzzi, J. L. Jr. & Jaffe, A. S. Cardiac troponin for assessment of myocardial injury in COVID-19: JACC review topic of the week. J. Am. Coll. Cardiol. 76, 1244–1258 (2020).
-
De Michieli, L. et al. High-sensitivity cardiac troponin T for the detection of myocardial injury and risk stratification in COVID-19. Clin. Chem. 67, 1080–1089 (2021).
-
Lala, A. et al. Prevalence and impact of myocardial injury in patients hospitalized with COVID-19 infection. J. Am. Coll. Cardiol. 76, 533–546 (2020).
-
Wilson, K. & Hawken, S. Drug prophylactic studies and measures of upshot using the self-controlled case serial design. Pharmacoepidemiol. Drug Saf. 22, 108–110 (2013).
-
Fonseca-Rodríguez, O. et al. Avoiding bias in self-controlled case series studies of coronavirus disease 2019. Stat Med. 40, 6197–6208 (2021).
-
Lipsitch et al. Negative controls: a tool for detecting confounding and bias in observational studies. Epidemiology 21, 383–388 (2010).
-
Kounis, North. G. Allergic reactions to electric current available COVID-19 vaccinations: pathophysiology, causality, and therapeutic considerations. Vaccines (Basel) 9, 221 (2021).
Acknowledgements
This project involves data derived from patient-level information collected by the National Wellness Service (NHS), every bit function of the care and support of cancer patients. The SARS-Cov-2 examination data are collated, maintained and quality assured by Public Health England (PHE). Access to the information was facilitated by the PHE Office for Data Release. The Hospital Episode Statistics, Secondary Users Service (SUS-PLUS) datasets and civil registration data are used by permission from NHS Digital who retain the copyright for that data. NHS Digital and PHE deport no responsibleness for the analysis or interpretation of the information. K.K. is supported by the National Plant for Wellness Research (NIHR) Applied Research Collaboration East Midlands (ARC-EM) and NIHR Lifestyle BRC. Grand.S.-H. is supported by the National Institute for Health Research Clinician Scientist Honor (NIHR-CS-2016-16-011). J.H.-C. and K.M.C. are supported by the NIHR Oxford Biomedical Enquiry Middle. N.50.Grand. and K.Thousand.C. are supported past the British Heart Foundation (Chair Awards CH/F/21/90010, CH/16/i/32013), Programme Grant (RG/20/ten/34966) and Enquiry Excellence Awards (RE/18/5/34216, RE18/3/34214). A.S. is supported past the Wellness Data Research United Kingdom Exhale Hub. This research is part of the Information and Connectivity National Cadre Report, led by Health Information Enquiry Britain in partnership with the office of National Statistics and funded by United kingdom of great britain and northern ireland Enquiry and Innovation (grant MC_PC_20029). The investigators admit the philanthropic support of the donors to the University of Oxford's COVID-19 Inquiry Response Fund. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the U.k. NIHR or the Department of Health. The funders of this study had no role in the design and carry of the study and did not review or approve the manuscript. The views expressed are those of the authors and not necessarily the funders. M.P., J.H.-C. and C.A.C.C. had full access to all the study data and J.H.-C. had final responsibleness for submission. This project is supported by a patient and public involvement advisory panel, which we give thanks for its connected support and guidance. The input of the panel has helped u.s. identify priority questions for consideration and likewise supported analysis. Patient and Public Involvement and Engagement advisers were supportive of the vital importance of reporting on cardiac risks associated with both vaccination against COVID-19 and COVID-19 itself.
Author information
Affiliations
Contributions
One thousand.P., J.H.-C. and C.A.C.C. led the study conceptualization, development of the enquiry question and analysis plan. J.H.-C. obtained funding, designed the analysis, obtained data approvals and contributed to interpretation of the analysis. M.P. undertook the data specification, curation, analysis. M.P. and N.L.M. wrote the commencement draft of the paper. S.D. undertook and reported on the Patient and Public Involvement and Date. L.H., 1000.M.C., F.Z., X.W.M., N.L.M., Chiliad.1000., One thousand.Due south.-H., P.W., A.H., S.D. and A.S. contributed to the discussion on protocol development and provided disquisitional feedback on drafts of the manuscript. All authors approved the protocol, contributed to the critical revision of the manuscript and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
A.Due south. is a member of the Scottish Government Principal Medical Officeholder'south COVID-xix Informational Group, the Scottish Government's Standing Committee on Pandemics and AstraZeneca'south Thrombotic Thrombocytopenic Informational Group. All roles are unremunerated. J.H.-C. reports grants from NIHR Biomedical Research Centre, Oxford, John Fell Oxford Academy Printing Research Fund and Cancer Research United Kingdom (CR-UK) grant no. C5255/A18085, through the CR-UK Oxford Centre, and grants from the Oxford Wellcome Institutional Strategic Support Fund (204826/Z/sixteen/Z) and other enquiry councils during the conduct of the report. J.H.-C. is an unpaid managing director of QResearch, a non-for-profit organization that is a partnership between the University of Oxford and EMIS Health who supplied the QResearch database used for this piece of work. J.H.-C. is a founder and shareholder of ClinRisk Ltd and was its medical manager until 31 May 2019. ClinRisk Ltd produces open up and closed source software to implement clinical adventure algorithms (exterior this piece of work) into clinical computer systems. J.H.-C. is chair of the NERVTAG risk stratification subgroup and a fellow member of Scientific Advisory Group for Emergencies COVID-19 groups and the NHS group advising on prioritization of use of monoclonal antibodies in SARS-CoV-2 infection. A.H. is a member of the Articulation Committee on Vaccination and Immunisation. Chiliad.Yard. is a member of the Governments Scientific Advisory Group for Emergencies. All other authors declare no competing interests related to this paper.
Additional information
Peer review data Nature Medicine cheers Karina Top, Leslie T. Cooper and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Jennifer Sargent was the primary editor on this article and managed its editorial process and peer review in collaboration with the residue of the editorial team.
Publisher'southward note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Supplementary data
Rights and permissions
Open Access This article is licensed under a Artistic Commons Attribution four.0 International License, which permits use, sharing, adaptation, distribution and reproduction in whatever medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other tertiary party material in this commodity are included in the commodity'due south Creative Eatables license, unless indicated otherwise in a credit line to the material. If cloth is not included in the commodity's Creative Eatables license and your intended use is non permitted by statutory regulation or exceeds the permitted apply, you lot volition need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
Reprints and Permissions
Nearly this commodity

Cite this article
Patone, Thou., Mei, X.W., Handunnetthi, L. et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-nineteen vaccination or SARS-CoV-two infection. Nat Med 28, 410–422 (2022). https://doi.org/10.1038/s41591-021-01630-0
-
Received:
-
Accustomed:
-
Published:
-
Issue Date:
-
DOI : https://doi.org/ten.1038/s41591-021-01630-0
Source: https://www.nature.com/articles/s41591-021-01630-0
0 Response to "Family Medicine Associates 15 Walnut S Hamilton Ma"
Post a Comment